BACKGROUND
Keloids generally present in a recognizable fashion, atypical locations may closely resemble other dermatologic conditions. Cutaneous sarcoidosis in particular can manifest as firm, infiltrated papules or plaques on the face and may mimic keloids both clinically and, in certain variants, histologically.
Keloids involving the nasal tip are exceedingly rare. To date, solitary keloids confined to the nasal tip have not been reported in the literature, making such cases diagnostically challenging and clinically notable. We describe an unusual instance of a nasal-tip keloid initially suggestive of cutaneous sarcoidosis, ultimately requiring histopathological confirmation for accurate diagnosis.
RESULTS
A 50-year-old man from Mali with Fitzpatrick phototype VI presented with a progressively enlarging, asymptomatic, firm, brownish papule located centrally on the nasal tip. His medical history was reviewed with particular attention to trauma and scarring tendencies. He reported undergoing surgical decortication for rhinophyma one year earlier but denied any other procedures, injuries, or a personal or family history of keloids.
The lesion was evaluated for size, color, consistency, and borders, and a complete cutaneous examination revealed no additional abnormalities (figure 1). Systemic symptoms commonly associated with sarcoidosis—such as dyspnea, chronic cough, arthralgia, fever, weight loss, or ocular manifestations—were assessed and absent.The initial clinical impression remained equivocal because the appearance of the papule was compatible with sarcoidosis, particularly considering its facial location.
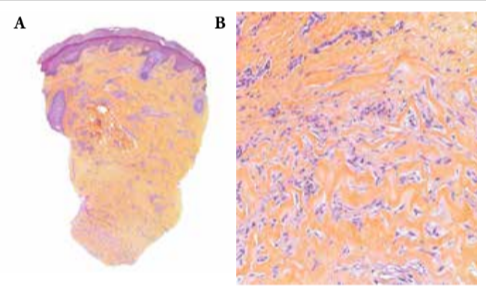
Given the uncertain diagnosis, a punch biopsy was performed. Microscopic examination of the biopsy specimen revealed dense dermal fibrosis composed of thickened, hyalinized collagen bundles occupying the deep dermis. Numerous fibroblasts and myofibroblasts were present between the collagen fibers, features consistent with a keloid. Importantly, no granulomatous infiltrate, epithelioid histiocytes, or multinucleated giant cells were identified (figure 2 A-B). Special stains demonstrated the absence of fungal organisms, acid-fast bacilli, and mucin deposition, excluding infectious and mucinous dermatoses. The combined findings supported a diagnosis of keloid and effectively ruled out sarcoidosis.
The patient showed no significant clinical improvement after several weeks of topical corticosteroid therapy. Considering the high recurrence rates associated with surgical excision—especially in cosmetically sensitive facial areas—a conservative management approach was maintained while evaluating potential alternatives such
as intralesional corticosteroids or multimodal therapeutic strategies.
DISCUSSION
This case illustrates an uncommon presentation of a keloid arising on the nasal tip, a site rarely associated with keloid formation. The patient’s prior surgical decortication for rhinophyma likely provided the initial traumatic event necessary to trigger abnormal wound healing. The rarity of keloids in this location, combined with the lesion’s firm and infiltrated appearance, explains why sarcoidosis was considered at presentation. The possibility of cutaneous sarcoidosis is particularly relevant in cases involving facial papules, which may be solitary and clinically indistinguishable from fibrotic lesions.
Keloids typically display an imbalance between collagen synthesis and degradation and an elevated type I to type III collagen ratio. Yet in atypical cases, such clinical patterns may be misleading. Histopathology was essential
in this case, demonstrating dense dermal fibrosis without granulomatous inflammation and ruling out infectious mimickers. This underscores the importance of biopsy when the clinical presentation deviates from classical patterns or when alternative diagnoses remain plausible.
Therapeutic management of facial keloids remains challenging. Intralesional corticosteroids are generally considered the first-line treatment but may offer limited efficacy in long-standing or dense lesions. Silicone-based therapies, laser treatment, and combination approaches may improve outcomes, although recurrence is frequent. Surgical excision carries an especially high risk of recurrence when performed alone, and for nasal-tip lesions, the cosmetic and structural implications must be carefully considered.
CONCLUSION
To our knowledge, this case represents the first reported instance of a nasal-tip keloid clinically mimicking cutaneous sarcoidosis. Its unusual localization and misleading appearance highlight the diagnostic difficulty associated with atypical keloids and demonstrate the crucial role of histopathology when clinical features are inconclusive. Accurate diagnosis helps avoid unnecessary systemic investigations and guides appropriate treatment in these rare and deceptive presentations.