
BACKGROUND
The biologically effective dose (BED) is a radiobiological method for comparing radiotherapy dose-fractionation schedules by converting total dose and dose per fraction into a common biological effect scale. This is based on the linear–quadratic (LQ) model for cell survival, from which an “α/ ratio” (i.e. the dose, in Gy, where the linear/single-hit and quadratic /multi-hit cell killing components of dose are equal) is determined for the tissue under consideration. The LQ model has proven to be robust across many tissues but uncertainty persists in keloid radiotherapy, both because fibroblasts are involved and because BED values for keloid treatment have frequently been reported without specifying whether they are calculated using α/ =10 (BED10), as employed in early radiobiological analyses, or 2.5 (BED2.5), as increasingly argued to be more appropriate for the post-excisional keloid bed. This ambiguity complicates interpretation of dose– response relationships and comparison between treatment regimens.
Further controversy concerns whether outcome is determined primarily by dose, radiation modality, fractionation schedule, timing of postoperative irradiation, or whether these factors converge within an optimal therapeutic BED window, consistent with Dale’s funnel model of radiobiological optimisation.
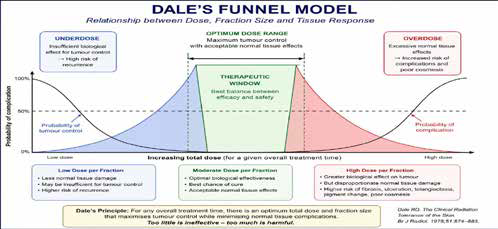
In this optimisation framework, underdosing risks recurrence, while, in the case of post- excisional keloids, over-escalation of dose may increase fibrosis, skin injury and produce poorer cosmesis, without improving control. Additional uncertainty exists regarding whether radiotherapy delivered within 24 hours of surgery is biologically and clinically necessary, although emerging wound healing biology suggests fibroblast repopulation may begin within 48 hours of excision.
This study therefore examines whether systematic review of treatment outcomes supports the hypothesis that recurrence control in excised keloids depends principally upon achieving an optimal BED window delivered sufficiently early postoperatively, with fraction number potentially of secondary importance once adequate timely biological dose is
achieved.
METHODS
A systematic comparative review was undertaken of outcome data for excised keloids treated with external beam radiotherapy, drawing on:
(i) Mankowski’s meta-analysis and its dose-fractionation subsets;
(ii) post-2017 reviews and meta-analyses examining: modality; BED; treatment timing; fractionation; recurrence; and adverse effects; and
(iii) mature treatment series reported through the 2nd–5th International Keloid Symposia and in related literature, using only final datasets where serial reports existed and patient numbers were large.
For each study, radiation modality (superficial X-ray or megavoltage electron beam), fractionation regimen, reported or recalculated BED (both BED2.5 & BED10 values, for retrospective transparency), recurrence rate, and follow-up duration were extracted and compared, recognising that one year, three year and five year recurrence outcomes are not interchangeable. Attention was particularly given to whether outcomes converged within an apparent therapeutic BED range and whether evidence supported treatment initiation within 24–48 hours post surgery.
RESULTS
Outcomes of post excisional keloid treatment are tabulated below:
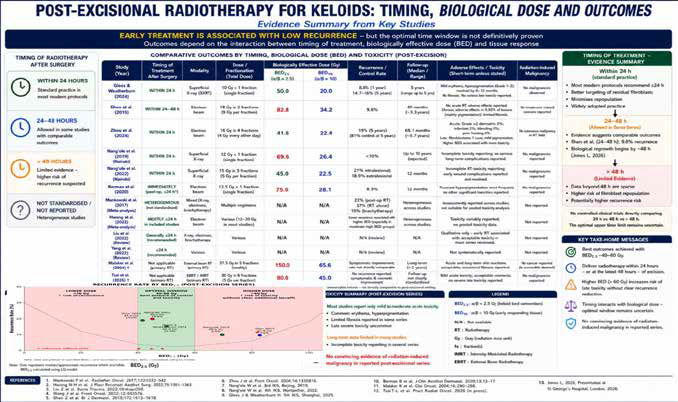
(Key series of results for radiotherapy treatment of unexcised keloids are also included to illustrate the difference in treatment regimens
employed and their treatment outcomes but are not otherwise analysed.)
CONCLUSION
Systematic review of available outcome data supports a model of BED guided optimisation, rather than simple dose escalation (e.g. up to a historically proposed BED10 = 30 Gy) or fraction-number selection, as a rational framework for post-excisional keloid radiotherapy. Current evidence suggests an effective therapeutic BED window may exist in which durable recurrence control can be achieved while
minimising toxicity, consistent with Dale’s funnel model.
A single 10 Gy fraction delivered within 24 hours appears to lie within this effective window between BED2.5 = 40 Gy and BED2.5 = 60 Gy and compares favourably with more fractionated regimens, when biological dose and follow-up maturity are considered. The evidence further suggests that ambiguity surrounding α/ assumptions has contributed substantially to confusion in the literature and that BED values should always be explicitly reported as BED2.5 or BED10.
While prospective comparative studies remain needed, present evidence increasingly supports the hypothesis that achieving an optimal BED window and treating early may matter more than fraction number per se.
REFERENCES
As listed beneath the relevant Figure.


