
BACKGROUND
Toe Keloid Disorder developing after syndactyly release is infrequently described but can be highly disruptive for pediatric patients due to symptoms, cosmetic burden,
and functional impairment related to interdigital tethering or progressive re adhesion.
Evidence guiding toe-specific management in children is limited, and many single- modality approaches provide incomplete control in anatomically constrained webspaces.
We evaluated a multimodal protocol integrating punch excision, fractional CO2 laser therapy, and intralesional pingyangmycin designed to (1) mechanically debulk and decompress thick toe Keloid Lesions, (2) remodel lesion architecture while releasing interdigital adhesion to improve mobility, and (3) locally suppress fibroproliferative activity. This study evaluated a multimodal protocol combining punch excision, fractional ablative remodeling (CO2 laser), and targeted intralesional chemotherapy (pingyangmycin), assessing its association with measurable improvement in clinical severity scores and an acceptable short-term safety profile.
METHODS
We conducted a retrospective study at two tertiary dermatology centers (Shenzhen Children’s Hospital and Dermatology Hospital of Southern Medical University). Pediatric patients with toe Keloid Lesions following syndactyly separation surgery were eligible if lesions were pathologically confirmed and the combined protocol was completed between January 2022 and January 2023 with documented follow- up. Baseline variables included age, sex, time from lesion development to treatment initiation, number of involved sites, and toe webspaces affected.
Intervention: Surface anesthesia was achieved using compound procaine/lidocaine cream, followed by tumescent local anesthesia with lidocaine plus epinephrine injected into lesions. Punch Excision was performed using a 2-mm disposable biopsy punch rotated into the Keloid Lesion at 5–10 mm intervals; cylindrical tissue segments were excised flush to the lesion base using tissue scissors to create multiple small cylindrical wounds across the lesion, aiming to reduce bulk and redistribute local mechanical tension. After hemostasis, fractional CO2 laser therapy was delivered with a CO2 device (JZ-2, Chengdu Guoxiong Photoelectricity Technology Co., Ltd.). A modulated pulse mode (2–4 W) was used for dot-matrix ablation at approximately 3-mm intervals, including careful removal of proliferative adherent tissue in the interdigital region to address functional limitation and reduce re-adhesio risk. A scanning mode was subsequently applied with non- overlapping spots (energy 15 mJ/cm2; spot center distance 1 mm; coverage 3%). Immediately after laser treatment, pingyangmycin (1%) mixed 1:1 with lidocaine (2%) was
injected intralesionally at multiple points. Post-procedure management included MEBO ointment applied 5 times daily until re-epithelialization. The complete combined procedure was performed twice at 3-month intervals. Between the two sessions, additional intralesional multi-point pingyangmycin injections were administered every 4 weeks.
Outcome assessment: Two independent physicians not involved in treatment evaluated each lesion using the Vancouver Scar Scale (VSS) domains (pigmentation/
color, thickness/height, vascularity, pliability) at baseline and one month after the final combined session; the mean of the two ratings was analyzed. Adverse events from the first procedure through one month after the final session were recorded, including infection, ulceration, erythema, pigmentary change, delayed healing, or lesion worsening. Statistical analyses were performed with SPSS 22.0; paired t-tests compared baseline and post-treatment VSS scores, with P < 0.05 considered significant.
RESULTS
Four pediatric patients (3 male, 1 female) with a mean age of 3.9 years were included. Time from lesion development to treatment initiation ranged from 4 months to 2 years (mean 10 months). Ten toe lesion sites were treated across the cohort, involving first–second and second–third toe webspaces, including bilateral involvement in one patient. At baseline, mean VSS component scores were 2.75 ± 0.50 (color), 3.25 ± 0.96 (thickness), 2.75 ± 0.50 (vascularity), and 3.50 ± 1.29 (pliability), yielding a total mean VSS score of 10.7 ± 1.34. One month after the final combined treatment, mean component scores improved to 2.25 ± 0.50 (color; P < 0.05), 1.75 ± 0.96 (thickness; P < 0.01), 1.75 ± 0.96 (vascularity; P < 0.01), and 1.50 ± 1.00 (pliability; P < 0.01). The total mean VSS score decreased to 5.2 ± 2.35 (P < 0.01), consistent with improvement across both visible and tactile domains(Table.1). No adverse events— including wound infection, ulceration, delayed wound closure, or post-inflammatory pigmentation changes—were observed during the treatment period or within one month after the last session.
CONCLUSION
In this retrospective pediatric cohort with toe Keloid Disorder after syndactyly release, a combined protocol of punch excision, fractional CO2 laser therapy, and
intralesional pingyangmycin was associated with improvement in overall clinical severity and multiple VSS domains, with an acceptable short-term safety
profile. This multimodal approach may be particularly useful for toe Keloid Lesions in anatomically constrained webspaces where debulking and mobility restoration are
clinical priorities. Key limitations include small sample size, retrospective design, and absence of long-term recurrence endpoints. Prospective studies with larger
cohorts, standardized functional measures (e.g., toe range of motion, webspace depth), and extended follow-up are warranted to evaluate durability, optimize dosing intervals, and compare this protocol with other multimodal strategies.
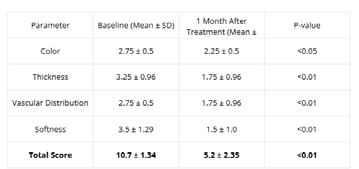
Table1.Clinical improvement according to the VSS scores at baseline and the follow -up.


